

If you have been feeling worse at home than anywhere else and cannot figure out why, mold exposure may be the reason. Mold exposure symptoms are the health effects produced when a person inhales, ingests, or contacts mold spores or mycotoxins indoors; according to the CDC and EPA, these effects range from mild nasal irritation to serious lung disease depending on exposure level and individual health status. Symptoms are frequently mistaken for a persistent cold, seasonal allergies, or unexplained fatigue, which means many people spend months treating the wrong problem.
Key insights
- Symptoms vary by mechanism. Mold causes health effects through three pathways: allergic reactions, non-allergic irritation, and mycotoxin exposure. Each produces a different symptom profile and requires a different response.
- Location is the biggest clue. Symptoms that worsen at home and improve elsewhere point strongly to an indoor environmental trigger. Keep a location-based symptom diary before your doctor visit.
- Onset can be fast or slow. Allergic individuals can react within minutes; non-allergic individuals may take weeks or months of cumulative exposure to develop symptoms.
- High-risk populations face more serious outcomes. Children, the elderly, people with asthma, and immunocompromised individuals can develop infections and permanent lung changes, not just allergy symptoms.
- Treating symptoms without removing mold is ineffective. Antihistamines and inhalers provide relief, but improvement is limited or short-lived if the source of exposure remains in the home.
- About 47% of U.S. residential buildings contain dampness or mold, according to NIEHS, meaning the exposure is far more common than most people realize.
How mold affects the body: three mechanisms
Mold causes health effects through three distinct biological pathways: allergic reaction, non-allergic irritation, and mycotoxin exposure. Understanding which one is operating matters because each produces a different symptom profile, affects a different population, and points toward a different response.
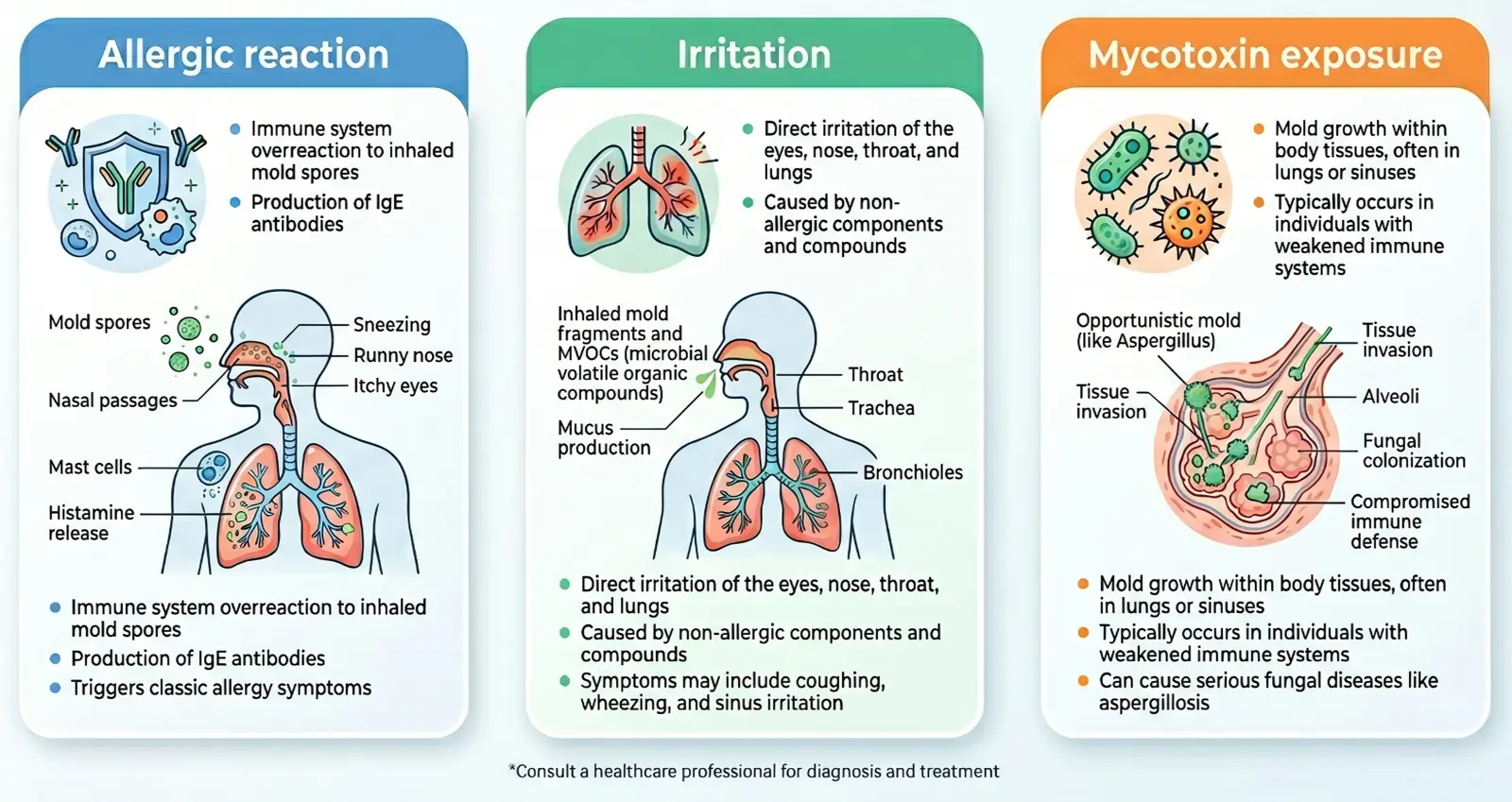
Allergic reaction. When the immune system identifies mold spores as a threat, it produces IgE antibodies that trigger histamine release on re-exposure, causing classic allergy symptoms within minutes to hours. This is the most common category and affects people who have been sensitized to specific mold species.
Non-allergic irritation. Mold spores and fragments can irritate the respiratory tract, eyes, and skin even in people who are not allergic, producing symptoms through direct physical and chemical aggravation rather than an immune response. This means some level of symptom risk exists for most people in heavily contaminated environments.
Mycotoxin exposure. Certain mold species produce mycotoxins, secondary metabolites that can cause systemic inflammatory responses in susceptible individuals, including effects on the neurological, musculoskeletal, and cognitive systems. In immunocompromised individuals, some species such as Aspergillus can also colonize lung tissue directly, causing serious fungal disease. This category affects a smaller percentage of people, though research from WHO and NIEHS confirms the association with damp indoor environments.
The mold health risks associated with each mechanism differ significantly in severity and treatment.
Symptoms of mold exposure by body system
Mold exposure produces symptoms across multiple body systems, with upper respiratory effects, including nasal congestion, sneezing, coughing, and wheezing, being the most common, followed by eye irritation, skin reactions, and in prolonged or high-level exposures, cognitive and systemic symptoms such as fatigue and brain fog. The table below organizes the full documented symptom range by body system, with severity context and the mechanism most likely responsible.

Symptoms vary widely between individuals. The same exposure level that causes mild sneezing in one person can trigger asthma attacks or skin reactions in another. Sensitivity depends on whether the person has a mold allergy, their underlying health conditions, and how long they have been exposed. People without any known allergies can still develop symptoms if mold concentrations are high enough or exposure is prolonged.
| Body system | Symptoms | Severity | Primary mechanism |
|---|---|---|---|
| Upper respiratory | Nasal congestion, sneezing, runny nose, postnasal drip, sinus pressure | Mild to moderate | Allergic, irritant |
| Lower respiratory | Coughing, wheezing, chest tightness, shortness of breath, asthma flare-ups | Moderate to severe | Allergic, irritant |
| Eyes | Itchy, red, or watery eyes; burning sensation | Mild to moderate | Allergic, irritant |
| Skin | Rash, hives, dry or itchy skin, contact dermatitis | Mild to moderate | Allergic, irritant |
| Cognitive / neurological | Brain fog, difficulty concentrating, memory lapses, headaches | Mild to severe | Mycotoxin, inflammatory |
| Fatigue | Persistent tiredness, weakness, low energy | Mild to severe | Mycotoxin, inflammatory |
| Musculoskeletal | Joint pain, muscle aches, morning stiffness | Moderate | Mycotoxin, inflammatory |
| Gastrointestinal | Nausea, bloating (less common) | Mild | Mycotoxin |
The most common symptoms in population studies are nasal congestion, coughing, wheezing, and eye irritation. The less common systemic symptoms, including fatigue, brain fog, and joint pain, are more often associated with prolonged exposure and mycotoxin-producing species, though the clinical evidence base for these associations is still developing.
According to the CDC: Basic Facts About Mold, mold can irritate the eyes, skin, nose, throat, and lungs even in individuals without mold allergies, meaning some level of symptom risk exists for most people in heavily contaminated environments.
How long does it take for mold to cause symptoms?
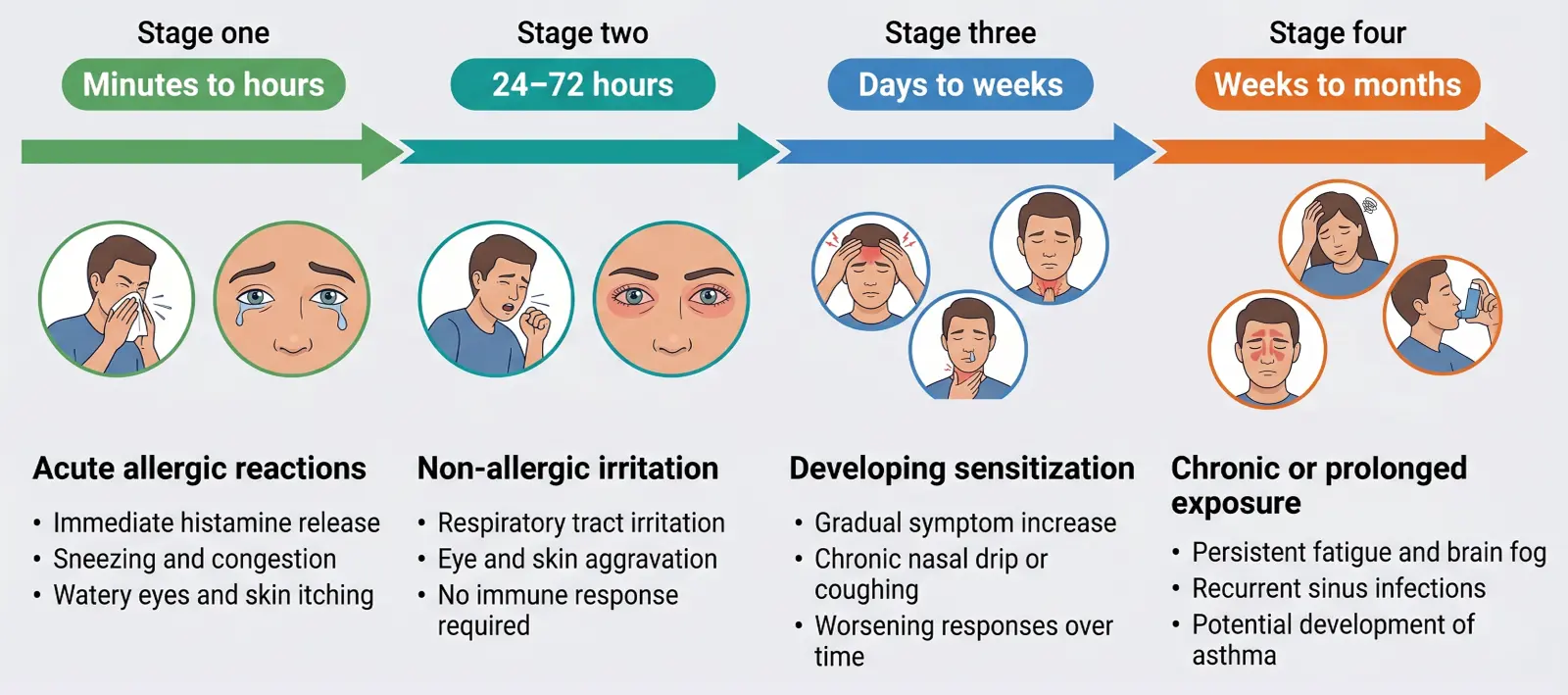
Mold exposure symptoms can appear within minutes in allergic individuals or take weeks to months to develop in people without allergies who face ongoing low-level exposure. Onset time varies based on mold species, spore concentration, and how long exposure has been occurring. For people without allergies, symptoms typically develop gradually over days, weeks, or months of repeated exposure as cumulative irritation and inflammatory responses build.
Acute exposure at high concentrations, such as disturbing a large mold colony during renovation, can cause rapid-onset respiratory symptoms and eye irritation in most people regardless of allergy status. Chronic low-level exposure in a home with hidden mold, including growth that developed after a water event, often produces a slower symptom progression that is easy to attribute to other causes. The mold after water damage guide covers how quickly mold can establish after a leak or flood.
- Minutes to hours: Allergic individuals upon entering a moldy space
- 24–72 hours: Non-allergic irritation after significant acute exposure
- Days to weeks: Gradual symptom onset with ongoing moderate exposure
- Weeks to months: Systemic symptoms from prolonged exposure in sensitive individuals
After leaving a contaminated environment, most allergic symptoms improve within 1–3 days. Recovery from hypersensitivity pneumonitis or prolonged exposure can take weeks to months and may require medical treatment.
Who is most at risk
People with asthma, chronic lung disease, or compromised immune systems face the most serious risk from mold exposure, along with children, the elderly, and pregnant women. Severity of symptoms is strongly influenced by individual health status, and the same level of mold exposure that produces mild congestion in a healthy adult can trigger a respiratory infection or permanent lung damage in a high-risk individual. The Institute of Medicine's 2004 report found sufficient evidence linking damp indoor environments to worsening asthma in people with pre-existing disease and evidence of association with new-onset asthma.

Children: Developing immune and respiratory systems respond differently to environmental exposures. Children in damp homes have documented higher rates of respiratory infections, asthma development, and allergic sensitization.
Elderly individuals: Aging immune systems have a reduced capacity to contain fungal pathogens, increasing risk of infection beyond typical allergic response.
People with asthma or chronic lung disease: COPD, chronic bronchitis, and pre-existing asthma significantly amplify vulnerability to both irritant effects and inflammatory responses.
Immunocompromised individuals: People undergoing chemotherapy, organ transplant recipients, or those with HIV/AIDS face risk of invasive fungal infections, including pulmonary aspergillosis, from prolonged mold exposure. The CDC notes that immunocompromised individuals may develop actual fungal infections in the airways rather than allergic reactions alone. Professional mold inspection is strongly recommended for any immunocompromised person with unexplained respiratory symptoms.
People with mold allergies: Allergic sensitization to mold species like Cladosporium, Aspergillus, Penicillium, and Alternaria significantly lowers the threshold for symptoms.
Pregnant women: Emerging evidence suggests heightened inflammatory sensitivity during pregnancy, though the research on mold-specific effects in this population is limited. Controlling moisture and humidity is the most effective protective measure across all high-risk groups; the mold prevention guide covers the core strategies.
Serious conditions linked to mold exposure
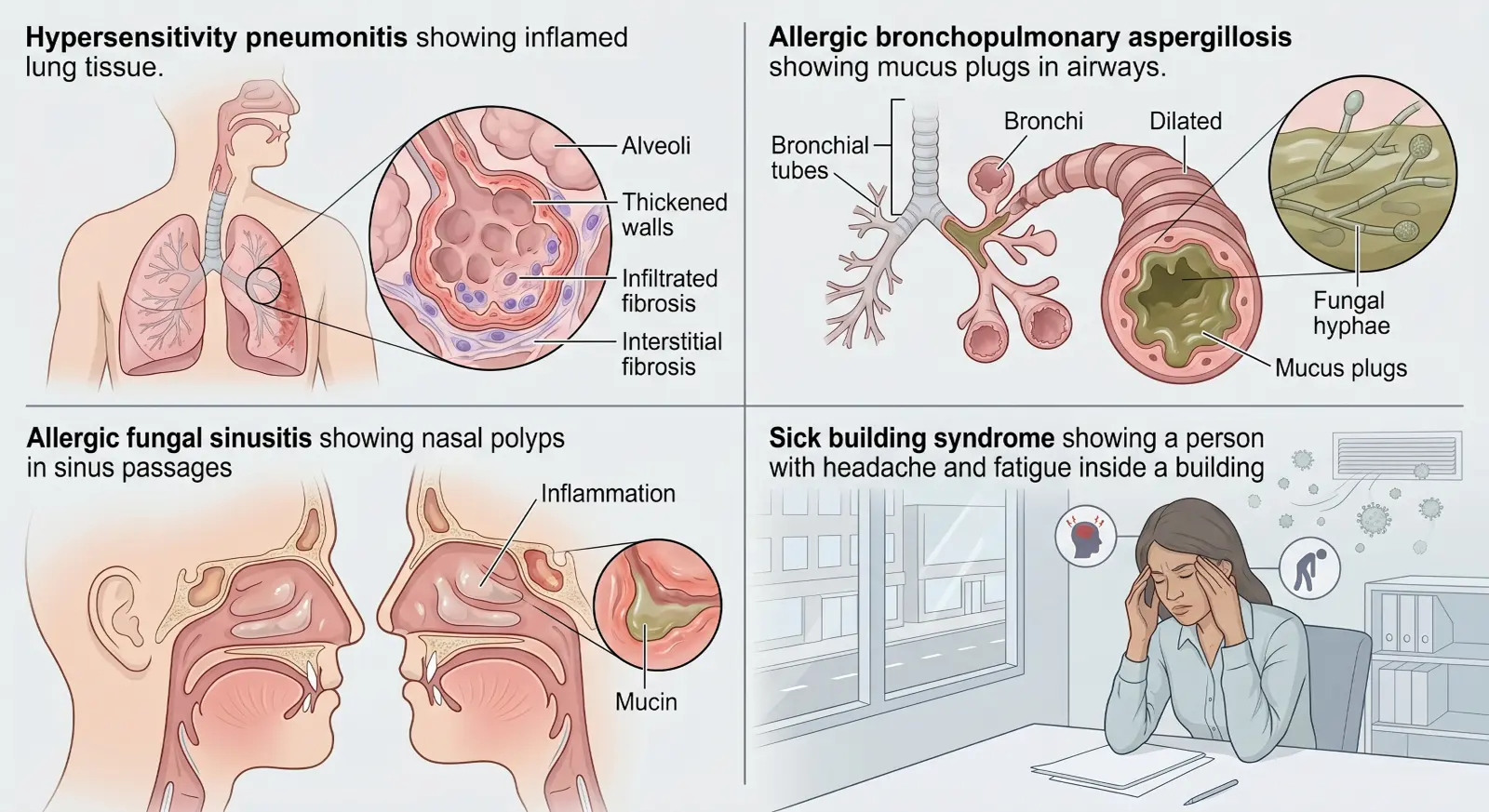
Prolonged or high-level mold exposure can progress beyond common allergy symptoms to four named medical conditions: hypersensitivity pneumonitis, allergic bronchopulmonary aspergillosis (ABPA), allergic fungal sinusitis, and sick building syndrome. Each requires physician involvement and will not resolve without removing the source of exposure alongside professional mold remediation.
While most mold-related health issues are relatively minor, certain individuals can develop serious respiratory conditions requiring medical attention. One of the most concerning conditions is hypersensitivity pneumonitis, an inflammatory lung disease that occurs when sensitive individuals inhale mold spores.
Hypersensitivity pneumonitis
Hypersensitivity pneumonitis is an inflammatory lung condition triggered by repeated inhalation of organic particles, including mold spores. It produces flu-like symptoms, shortness of breath, and fever that typically improve when leaving the exposure environment. With continued exposure, persistent lung inflammation can progress to permanent fibrosis. The CDC/NIOSH has documented cases in workers in water-damaged buildings with contaminated HVAC systems and roof or plumbing leaks.
Allergic bronchopulmonary aspergillosis (ABPA)
ABPA is a hypersensitivity reaction to Aspergillus species that occurs primarily in people with asthma or cystic fibrosis. It causes worsening asthma, productive cough with brownish mucus plugs, and fever. Left untreated, ABPA can cause bronchiectasis and permanent lung damage.
Allergic fungal sinusitis
This chronic sinusitis variant is driven by a hypersensitivity response to airborne fungi. Symptoms include persistent sinus pressure, thick colored mucus, nasal polyps, and facial pain. It is often misdiagnosed as bacterial sinusitis and treated repeatedly with antibiotics without improvement.
Sick building syndrome
Sick building syndrome describes a pattern of symptoms, including headaches, fatigue, respiratory irritation, and difficulty concentrating, that are linked to time spent in a specific building and improve when leaving. Mold and mycotoxins from water-damaged materials are among the documented contributors, per NIOSH research on dampness in buildings.
The location pattern test: a key diagnostic clue
One of the most useful self-assessment tools for mold-related illness is tracking where and when symptoms occur. Symptoms that follow a clear location pattern are a strong signal that an environmental source is involved. Ask yourself:

Track your symptoms carefully over several weeks to identify meaningful patterns. The most revealing question to ask yourself is simple but powerful.
- Do symptoms consistently worsen at home and improve after a day or two away?
- Do symptoms flare in a specific room but not others?
- Have others in the household reported similar symptoms?
- Did symptoms start after a water event such as a leak, flood, or prolonged humidity problem?
- Does returning home reliably bring symptoms back?
If the answer to two or more of these questions is yes, a professional mold inspection with moisture mapping is the appropriate next step, even if you have not seen visible mold. Many of the most problematic mold situations involve growth behind walls, under flooring, or inside HVAC systems, where there are no obvious visual signs. The signs of mold in a home often include musty odors before any visible growth is apparent.
When to see a doctor
Consult a physician if respiratory symptoms, persistent fatigue, or recurring sinus infections do not resolve within two weeks, or if symptoms follow a clear pattern of worsening at home and improving away from it. High-risk individuals including those with asthma, COPD, or a compromised immune system should seek care at a lower threshold than otherwise healthy adults. Understanding when mold remediation is required is a parallel decision that should happen alongside seeking medical care.

You should consult a physician if you experience any of the following:
- Respiratory symptoms including wheezing, chest tightness, or shortness of breath
- Symptoms that persist for more than two weeks without an obvious cause
- A worsening pattern despite treatment with over-the-counter allergy medications
- Recurring sinus infections that do not resolve fully with antibiotics
- Symptoms that are clearly linked to a specific building or home
- Fever, night sweats, or coughing up blood (these require prompt evaluation)
- A known mold problem in your home combined with new or worsening respiratory symptoms
- Active water damage with visible mold spread, which warrants emergency mold removal alongside medical care
The EPA's mold guidance specifically recommends that high-risk individuals avoid being present during mold cleanup activities.
How doctors diagnose mold-related illness
Diagnosis of mold-related illness combines symptom history, physical examination, exposure context, and targeted tests. There is no single test that confirms "mold illness" as a unified diagnosis, because the health effects of mold span multiple mechanisms and conditions.

Skin prick test: The most common method for identifying mold allergies. A small amount of mold allergen is applied to the skin via a lancet prick. A raised wheal within 15 minutes indicates allergic sensitization to that species. Results are typically available within an hour.
Specific IgE blood test: Measures IgE antibodies in the blood that are specific to mold allergens. Useful when skin testing is not possible. Results take several days to return from the lab.
Pulmonary function tests: Spirometry and bronchodilator responsiveness testing assess airway obstruction and reversibility, helping confirm asthma diagnosis and severity. Relevant when wheezing or chest tightness is a primary complaint.
Imaging: Chest X-ray or CT scan may be ordered when hypersensitivity pneumonitis or ABPA is suspected. These can show ground-glass opacities, mucus plugging, or bronchiectasis in advanced cases.
Nasal endoscopy: Used when allergic fungal sinusitis is suspected, allowing direct visualization of polyps and fungal debris in the sinus passages.
Tell your doctor about any known water damage, musty odors in your home, or recent flooding history. This context is often the critical piece that connects a symptom pattern to an environmental source.
Treatment options for mold exposure symptoms
Treatment for mold exposure symptoms targets the specific mechanism involved: antihistamines and intranasal corticosteroids for allergic reactions, bronchodilators and inhaled corticosteroids for asthma, and antifungals or oral corticosteroids for serious conditions like ABPA or hypersensitivity pneumonitis. Removing the source of mold exposure is the most important step, because symptom treatment alone produces limited improvement if exposure continues.

For individuals experiencing allergic reactions to mold, several over-the-counter and prescription medications can help manage symptoms effectively. The following table outlines common treatment options and their specific applications:
| Treatment | Used for | Notes |
|---|---|---|
| Intranasal corticosteroid sprays | Allergic rhinitis, nasal congestion | First-line treatment; prescription and OTC options available |
| Antihistamines | Sneezing, itching, watery eyes | OTC options include cetirizine, loratadine, fexofenadine |
| Bronchodilators (inhalers) | Asthma symptoms, wheezing | Short-acting for acute relief; long-acting for ongoing asthma |
| Inhaled corticosteroids | Persistent asthma from mold exposure | Used for ongoing airway inflammation management |
| Antifungal medications | Invasive fungal infections, ABPA | Prescription only; used in immunocompromised patients or confirmed fungal infection |
| Allergen immunotherapy | Mold allergy desensitization | A series of allergy shots over 3–5 years; only for specific mold species |
| Nasal saline irrigation | Sinus congestion, postnasal drip | Daily use can clear allergens and reduce symptoms |
| Oral corticosteroids | Acute hypersensitivity pneumonitis, ABPA | Short-term use to reduce lung inflammation; physician-supervised |
According to Mayo Clinic's mold allergy guidelines, allergen immunotherapy can be effective for certain mold species but is not used for all types. Immunotherapy addresses allergic sensitization; it does not reduce exposure, which remains the priority.
Next steps at home
Treating symptoms medically without addressing the moisture source that feeds mold growth provides only partial and temporary relief. The steps below apply alongside any medical treatment and address the problem at its origin.
1. Document your symptoms
Keep a log of symptom type, timing, location, and severity for at least two weeks before your doctor visit. Note whether symptoms improve when away from home overnight or on vacation.
2. Identify moisture sources
Water intrusion from leaking pipes, condensation, poor ventilation, or past flooding is almost always the underlying cause of indoor mold. Visible water stains, peeling paint, or persistent musty odors are physical indicators.
3. Check high-risk areas
Mold in the bathroom concentrates in shower grout, caulk seams, and around toilet bases. Basements, attics, crawl spaces, and HVAC systems are other common sites. Not all mold is visible; growth inside walls, under flooring, and within ductwork is common.
If visible mold covers more than 10 square feet, a professional mold inspection with moisture mapping is appropriate before attempting any cleanup. For smaller areas, the EPA permits DIY mold removal on non-porous surfaces with proper PPE, though anyone in a high-risk category should not perform cleanup personally. Larger jobs, hidden mold, or any mold in HVAC systems require a licensed contractor.
Frequently asked questions
What are the most common symptoms of mold exposure?
The most common symptoms are nasal congestion, sneezing, coughing, itchy or watery eyes, and throat irritation. People with asthma or existing mold allergies may also experience wheezing and chest tightness. These symptoms closely resemble seasonal allergies, which is why mold exposure is frequently overlooked as the cause.
How quickly do mold exposure symptoms appear?
People with mold allergies can develop symptoms within minutes to hours of entering a moldy environment. Non-allergic individuals may not notice symptoms for days or weeks of repeated exposure. Onset depends on mold species, spore concentration, and individual sensitivity.
Can mold cause fatigue and brain fog?
Yes. Fatigue, difficulty concentrating, and brain fog are reported with prolonged mold exposure, particularly in individuals exposed to mycotoxin-producing species. A 2013 study in the journal Toxins found an association between mycotoxin exposure and chronic fatigue symptoms.
How do I know if mold is making me sick?
Track the location pattern: symptoms that consistently worsen at home and improve when away suggest an indoor environmental trigger. Combining this observation with a professional mold inspection is the most reliable way to confirm the connection.
Do symptoms go away after leaving the home?
For most allergic reactions, symptoms improve within 1–3 days away from the source. Recovery from hypersensitivity pneumonitis or prolonged systemic exposure may take weeks and often requires medical treatment.
What should I do if I think mold is causing my symptoms?
See a doctor to document your symptoms and discuss exposure history. Have your home inspected for mold at the same time. Treating symptoms without removing the source typically provides limited improvement.
Can children get sick from mold exposure?
Yes. Children are a high-risk group. The IOM found sufficient evidence linking damp indoor environments to respiratory infections, asthma exacerbation, and new-onset asthma in children. Their developing respiratory and immune systems make them especially vulnerable to prolonged exposure.
Sam Hickerson is the founder of RestoreAdvisor and writes consumer guides on mold remediation, inspection, testing, and home recovery. His work focuses on helping homeowners understand costs, risks, and when to call a professional. He draws on guidance from the EPA, CDC, IICRC, and other authoritative sources to make complex home issues easier to navigate.